Introduction: Two Standards, One Scheduling Problem
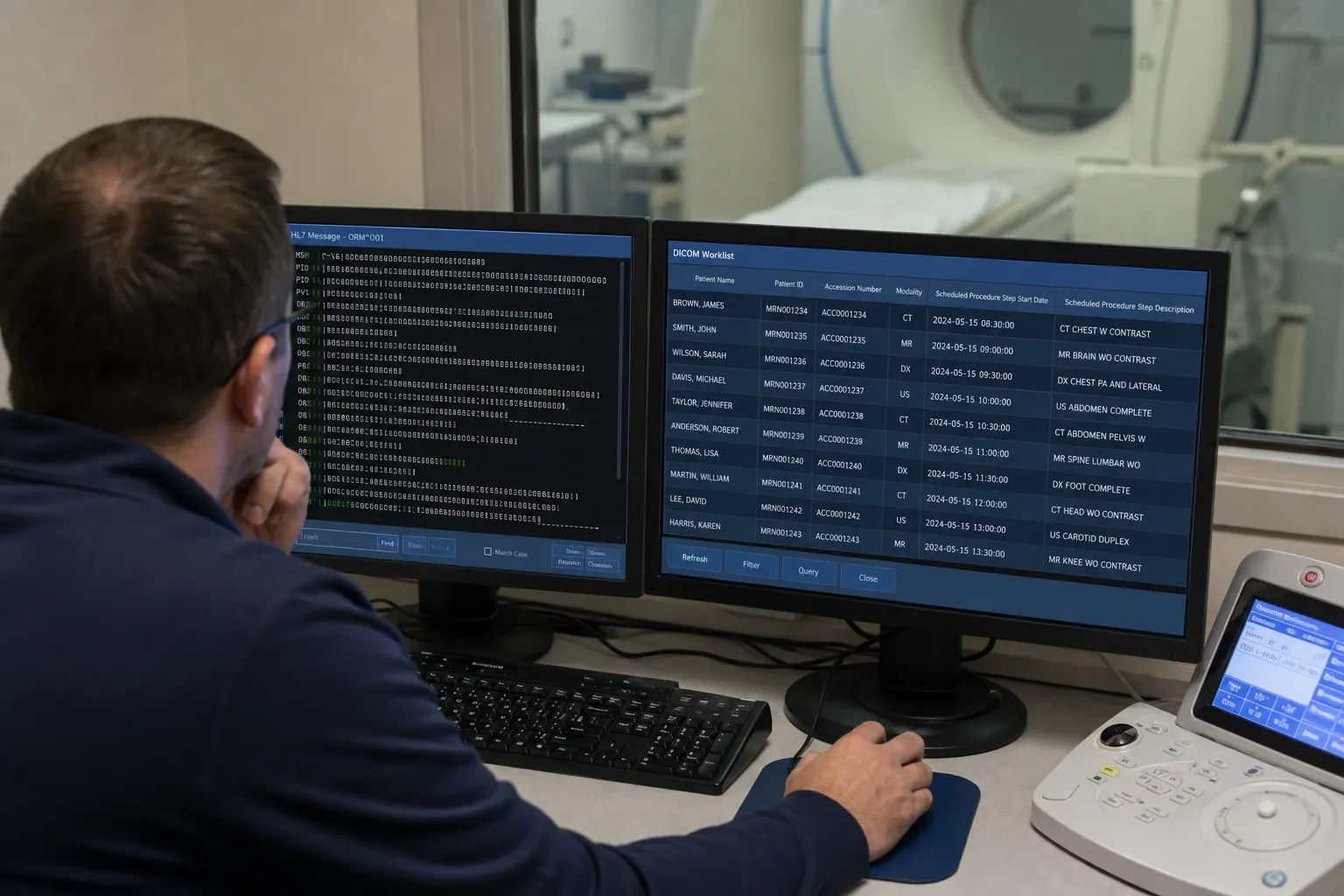
Radiology departments often talk about “the worklist” as if it were a single thing, but in technical reality two different standards usually cooperate to make imaging orders appear correctly at the scanner. On one side is the HL7 ORM message, which carries order-entry information from the EHR or RIS. On the other side is the DICOM Modality Worklist service, which lets the modality query a DICOM system for scheduled procedures. Both are essential, but they solve different parts of the workflow. Confusing them leads to poor interface design, duplicate logic, and avoidable go-live failures.
The distinction matters because radiology operations depend on precise alignment between patient demographics, accession numbers, procedure codes, and scheduled procedure steps. If the HL7 order arrives but the worklist entry is incomplete, technologists may type patient information manually. If the DICOM worklist is configured correctly but the upstream HL7 ORM mapping is wrong, the modality can retrieve the wrong description or no exam at all. Understanding which standard owns which responsibility is one of the highest-value pieces of knowledge in radiology integration.
This guide compares HL7 ORM and DICOM Modality Worklist in practical terms: what each standard contains, how they interact, where each one fits in RIS/PACS architecture, and how to choose the right troubleshooting path when exams fail to appear correctly. For hands-on analysis, you can inspect messages in our HL7 Viewer and experiment with order-to-worklist logic in the HL7 Radiology Worklist Builder.
What HL7 ORM Messages Do
An ORM^O01 message is the standard HL7 v2.x vehicle for communicating order-entry information. In radiology, the order is usually created in the EHR or RIS and contains the clinical request: who the patient is, what study was requested, when it was ordered, who ordered it, and what identifiers should be used downstream. The message commonly includes MSH for header data, PID for patient demographics, PV1 for visit context, ORC for common order control, and OBR for the actual requested procedure.
The key point is that ORM exists in the enterprise messaging layer. It is designed to move data between business systems such as EHRs, RIS platforms, scheduling systems, billing systems, and interface engines. It tells downstream systems that an order exists and carries the identifiers needed to manage it. It does not by itself define how a modality console will query and retrieve a worklist entry at scan time.
That is why ORM is necessary but not sufficient. You can have a perfectly valid radiology order moving through HL7 while the modality still shows an empty worklist because no DICOM MWL provider translated that order into a modality-queryable entry.
What DICOM Modality Worklist Does
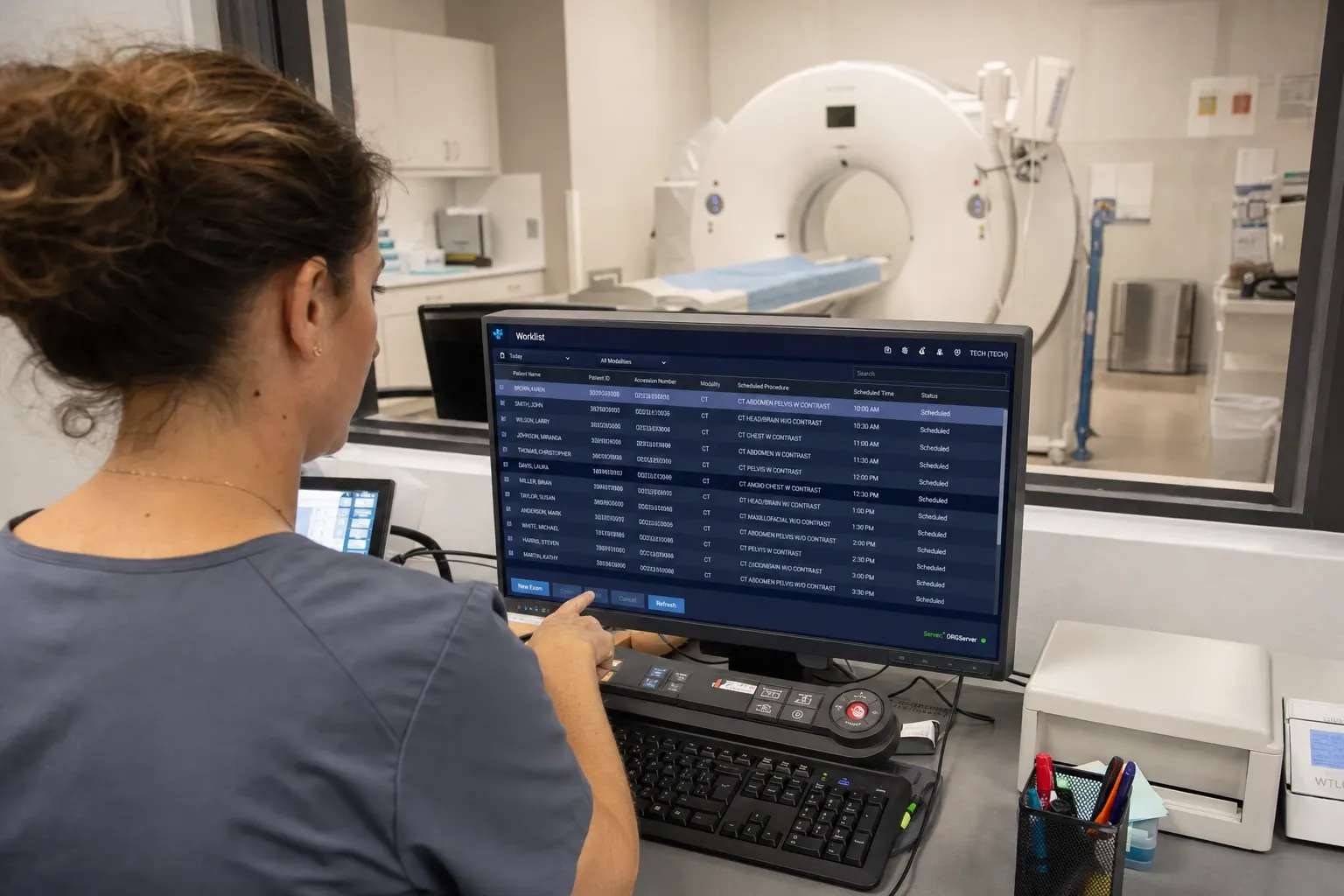
DICOM Modality Worklist is a DICOM query service, not a message in the HL7 sense. The modality acts as a client and sends a C-FIND request to a worklist provider, which may be the RIS, PACS, broker, or dedicated workflow engine. The response contains scheduled procedure information formatted in DICOM attributes such as Patient Name, Patient ID, Accession Number, Requested Procedure Description, Scheduled Procedure Step Start Date, and Modality.
The practical purpose of Modality Worklist is to eliminate manual re-entry at the scanner. Instead of typing patient demographics and exam information directly on the modality console, the technologist selects an existing worklist item. That improves efficiency, reduces demographic errors, and increases the chance that the acquired images will match the correct order and accession downstream.
In other words, HL7 ORM tells enterprise systems that an order exists. DICOM MWL makes that order consumable by the scanner.
Why Both Standards Coexist
The two standards coexist because radiology workflows span two technical worlds. Hospital information systems, scheduling applications, and interface engines have historically used HL7 v2.x. Imaging devices and PACS ecosystems use DICOM. Rather than forcing modalities to become native HL7 consumers, the architecture usually inserts a broker or RIS component that receives ORM messages, interprets them, and exposes the relevant subset through a DICOM worklist service.
This split is not redundant; it is a division of labor. HL7 excels at enterprise events and order management. DICOM excels at imaging-specific object structure and modality interaction. Trying to replace one entirely with the other usually means pushing complexity into the wrong part of the stack. A modality should not have to parse HL7 order messages directly, and an EHR should not need to speak DICOM C-FIND to create a radiology request.
For integration architects, the design question is therefore not “which standard is better?” but “where is the translation boundary and how is consistency enforced across it?”
Core Data Elements: Where the Same Information Appears Differently
The same business concepts appear in both domains, but in different shapes. Patient identity may originate in PID-3 and PID-5 in HL7, then appear as Patient ID and Patient Name in the DICOM worklist response. The accession number often starts in ORC or OBR and later appears in DICOM accession fields. Requested procedure codes or descriptions may originate in OBR-4 and map to Requested Procedure Description or Scheduled Procedure Step Description in the worklist response.
The challenge is not just field mapping but semantic alignment. If your HL7 side uses local procedure codes, who maps them to modality-facing descriptions? If your RIS supports multiple Scheduled Procedure Steps for a single order, how are those represented? If a mobile X-ray device only filters by modality and date, how much information must the MWL provider include to make selection safe for the technologist?
These questions are why radiology interface teams need both HL7 knowledge and DICOM workflow knowledge. A field-level comparison in an HL7 Viewer is often the first step, but the worklist response still has to be validated in the modality or DICOM-side tooling.
When HL7 ORM Is the Main Integration Surface
HL7 ORM is the primary integration surface when the goal is moving orders between enterprise systems. That includes EHR-to-RIS order entry, downstream notification to billing or scheduling, order updates and cancellations, and reporting to analytics or workflow engines. If the problem is that the RIS never received the order, the modality worklist is not your first troubleshooting surface. The right place to look is the HL7 feed, the interface engine, acknowledgment handling, and field mapping in ORC/OBR.
Typical HL7-centric incidents include missing OBR segments, wrong placer or filler numbers, incorrect patient-class routing, malformed provider IDs, duplicate orders, and canceled orders that never propagated. These are message-domain issues. They may later impact the worklist, but the root cause sits upstream in HL7 flow design.
That is exactly why a decoded message viewer is valuable. It lets analysts confirm what the source system actually sent before they start blaming the worklist service or the modality.
When DICOM MWL Is the Main Integration Surface
DICOM Modality Worklist becomes the primary surface when the order exists in the enterprise systems but the scanner cannot retrieve or use it correctly. Common symptoms include: the expected exam does not appear on the modality console, demographics look incomplete or stale, descriptions are ambiguous, the accession number is wrong, or multiple similar entries make safe selection difficult. In these cases the HL7 order may be perfectly fine; the problem lies in transformation, worklist population, filtering, or DICOM query behavior.
Typical MWL-side issues include wrong AE Title targeting, misconfigured query filters, Scheduled Procedure Step attributes not being populated, date formatting mismatches, multiple-step orders collapsed incorrectly, and modality type mismatches that cause the exam to be hidden. These are DICOM-workflow issues, even though the root data may have originated in HL7.
The key troubleshooting skill is knowing when to pivot. If the ORM never arrived, stay in HL7. If the ORM arrived and the scanner still has no usable exam, move to MWL inspection.
Design Patterns in Real Radiology Environments
In many hospitals the RIS acts as the worklist authority. It receives HL7 ORM messages, creates internal scheduling records, and exposes them to modalities through DICOM MWL. In other environments, an interface engine or broker sits between RIS and modality, normalizing orders and producing MWL responses. Large imaging networks may also use workflow brokers to merge site-specific codes, modality naming rules, and enterprise scheduling policies.
No matter the topology, one principle holds: the worklist is downstream of order management. The MWL provider should not invent business meaning that does not exist upstream. If the HL7 order lacks enough detail to generate a safe worklist entry, the answer is not creative DICOM coding; it is fixing the order-content requirements and the HL7 mapping.
That is also why governance matters. Radiology departments need agreement on which identifiers are canonical, which procedure description is displayed to technologists, and how cancellations, add-ons, and reschedules are handled across both standards.
Common Failure Modes and How to Diagnose Them
A classic failure mode is a valid HL7 order with a missing or weak OBR-4 universal service identifier. The order reaches the RIS, but the worklist provider cannot derive a useful modality-facing description. Another common issue is inconsistent accession-number assignment: one system treats ORC-2 as primary, another expects OBR or filler IDs, and the worklist entry ends up mismatched with the later images.
Cancellations are another trap. The HL7 side may send order-control updates correctly, but the worklist cache on the modality or broker side may not refresh, so a canceled study still appears selectable. On the DICOM side, query filters and scheduled-step dates often produce hidden exams that exist but never match the scanner search pattern. These patterns are why radiology troubleshooting is rarely solved by looking at only one standard.
A good rule is to compare three artifacts together: the original ORM message, the transformed order record in the receiving system, and the final MWL response visible to the modality. That chain reveals where meaning was lost.
Choosing the Right Tooling
For HL7 analysis, you need a field-aware message viewer that can decode PID, ORC, and OBR cleanly, highlight order identifiers, and expose repetitions without forcing analysts to count pipes manually. Our HL7 Viewer is designed for exactly that. For workflow modeling and synthetic validation, the HL7 Radiology Worklist Builder helps teams test how order data should be converted into modality-consumable worklist entries.
Those tools are complementary. One helps you inspect what happened. The other helps you reason about what should happen. Used together, they reduce the gap between interface analysts, RIS teams, and modality specialists.
Conclusion
HL7 ORM and DICOM Modality Worklist are not competing standards. They are sequential layers in the same radiology workflow. ORM carries order intent through enterprise messaging systems. DICOM MWL turns that order into something a modality can query and select safely at acquisition time. If you use the wrong tool to debug the wrong layer, you lose hours. If you understand the boundary between them, most radiology integration problems become much easier to isolate.
When exams fail to appear correctly, start by asking: is the problem upstream order communication or downstream modality presentation? Inspect the order in the HL7 Viewer, then validate the expected worklist behavior in the HL7 Radiology Worklist Builder. That one-two workflow is often the shortest path to a stable radiology interface.