Introduction: ORU Messages Carry Clinical Meaning That Must Survive the Transformation
ORU result interfaces look deceptively simple because the source message is usually shorter than a full ADT workflow and the target resources have obvious names: DiagnosticReport and Observation. Yet ORU mappings fail in production every day because result messages carry a mix of panel-level context, test-level coding, value typing, abnormal flags, narrative text, reference ranges, performer details, specimen context, and local code systems that are easy to flatten incorrectly.
When a team says it wants to convert ORU to FHIR, what it usually means is that it wants clinical results to become searchable, consumable, and reusable through modern APIs without losing the semantics that downstream clinicians, analytics teams, and decision support rules depend on. If you want to inspect the raw source message first, use our HL7 Viewer. If you want to experiment with the result bundle itself, the HL7 v2 to FHIR Mapper provides a fast way to compare OBR and OBX content with generated FHIR output.
This article focuses specifically on ORU^R01 mapping to DiagnosticReport and Observation. It complements our broader HL7 v2 to FHIR migration guide and pairs naturally with the companion article on ADT to Patient and Encounter mapping. Together they cover the two most common modernization paths: events that describe the patient journey and results that describe what clinicians learned from that journey.
DiagnosticReport Versus Observation: Get the Boundary Right
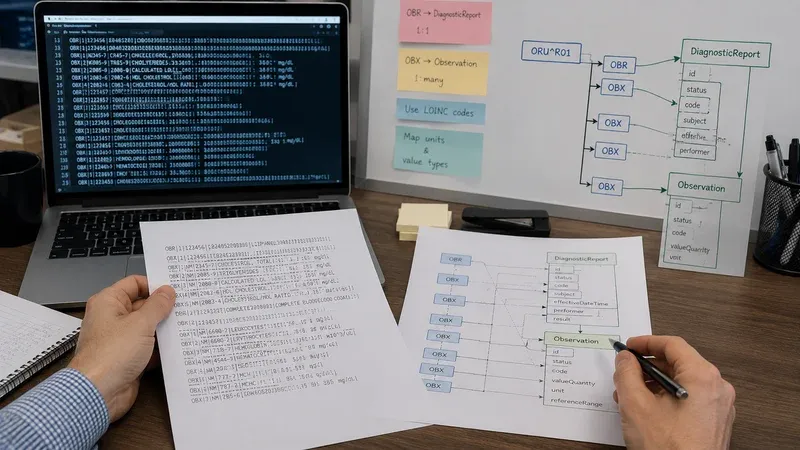
The most important conceptual distinction in ORU mapping is that a DiagnosticReport represents the reportable event or panel context, while each Observation represents an individual result. Many teams initially try to push everything into Observation because OBX segments feel like the center of the message. That loses the grouping context that FHIR expects and makes report-level search, audit, and display harder.
A good rule is to treat OBR as the anchor for DiagnosticReport and OBX segments as children that become Observation resources referenced from DiagnosticReport.result. If the message contains multiple OBR groups, you likely need multiple DiagnosticReport resources, each with its own Observation set. This grouping matters for lab panels, microbiology batteries, imaging reports with impression text, and any workflow where one accession or order leads to several discrete results.
OBR Segment to DiagnosticReport
OBR-4 Universal Service Identifier is usually the first mapping target. It becomes DiagnosticReport.code and should preserve the test or panel code, display text, and code system where possible. If the source sends LOINC, keep it as LOINC. If it sends a local code, preserve that too rather than pretending everything is standard. Honest coding beats false normalization because it lets downstream consumers understand exactly what data they received.
OBR-7 and OBR-22 often influence timing fields such as effectiveDateTime or issued depending on the source system's conventions. OBR-25 result status usually drives DiagnosticReport.status. Map status conservatively: final results should become final, corrected results should become corrected, and cancelled messages should not silently appear as final. If your source sends partial or preliminary states, preserve them rather than collapsing everything into final for convenience.
DiagnosticReport.subject often references the Patient derived from PID, and DiagnosticReport.encounter may reference the visit context if the message includes PV1. That is where coordination with your ADT strategy matters. If your patient and encounter identity model is weak, ORU mappings will struggle to connect results to the right longitudinal context. That is one reason this guide pairs closely with our ADT mapping article.
OBX Segment to Observation
Each OBX usually becomes one Observation. OBX-3 maps to Observation.code and should preserve the local or standard code used by the source system. OBX-11 maps to Observation.status, but do not assume OBX status and OBR status are always identical. An amended panel may contain observations with different business history from the overall report, especially in corrected or partially repeated workflows.
The decisive field is OBX-2 Value Type. It tells you how to interpret OBX-5. Numeric values often become valueQuantity. Text values may become valueString or, in some narrative-heavy workflows, a note or textual presentation. Coded results often become valueCodeableConcept. Date or timestamp results may become valueDateTime. Structured numeric types sometimes require range or comparator handling. A production-grade mapper should branch on OBX-2 explicitly instead of trying to coerce every value into a string.
OBX-6 units usually populate Observation.valueQuantity.unit, and if the source unit is a valid UCUM expression, preserve that coding explicitly. OBX-7 reference range may map to Observation.referenceRange, while OBX-8 abnormal flags often map to Observation.interpretation. These fields are not cosmetic. Clinical dashboards, alerting logic, and analytics often depend on them.
Value Type Patterns That Matter in Real Interfaces
Numeric laboratory results are the cleanest scenario, but even they have traps. If OBX-5 contains a number and OBX-6 contains units, use valueQuantity. Preserve decimal precision and do not round unless a downstream profile explicitly requires it. If the source sends less-than or greater-than qualifiers through a structured numeric type, do not strip the comparator. FHIR can model comparator semantics, and losing them changes clinical meaning.
Textual results are more variable. Narrative pathology comments, microbiology interpretations, and radiology impressions may come in TX or FT fields that are too rich to treat as simplistic measurements. Sometimes they still belong in Observation.valueString; sometimes they fit better into DiagnosticReport.conclusion or presentedForm, depending on how the source organizes the report. The key is to preserve report-level narrative separately from discrete analyte-level findings where possible.
Coded observations deserve special care because local code systems dominate many production labs. If OBX-5 contains a coded answer and the coding system is local, keep it local and add display text faithfully. Do not invent LOINC or SNOMED codings that were not sent. The receiving ecosystem can always build terminology translation later, but it cannot recover provenance if the original coding is overwritten.
Parent Child Structure, Panels, and Repeating Observations
Panels are where simplistic ORU mappers often break down. One OBR may describe a complete metabolic panel, while each OBX beneath it holds a specific analyte. In FHIR, that generally means one DiagnosticReport with multiple Observation references. If the source uses nested observation structure or sub-IDs to show grouped components, you may need Observation.hasMember or component modeling rather than a flat list. The right answer depends on whether each result has its own identity and interpretation or is merely a component of a single clinical measurement.
Microbiology and pathology can be even harder because one ORU may include organism findings, susceptibility data, comments, and amended status updates. Resist the urge to over-simplify. Your first goal is fidelity, not elegance. A FHIR structure that is slightly verbose but semantically faithful is far safer than a neat structure that drops the difference between a culture-level finding and an antibiotic-level susceptibility result.
Status, Corrections, and Result Lifecycle
Result lifecycle handling is not optional. ORU interfaces routinely send preliminary, final, corrected, and cancelled updates. If the receiver treats every ORU as a brand-new final report, clinicians and downstream applications can see stale or duplicated information. Build correlation logic that can find the existing DiagnosticReport and Observation records by business identifiers before deciding whether the new message creates, supersedes, or amends the previous result set.
That correlation logic often depends on placer or filler order numbers from ORC and OBR fields, accession identifiers, or local result identifiers. Whatever key you choose, it should be documented and tested. A corrected result must update the right record lineage. Otherwise you can end up with both the old and new values marked final, which is one of the most dangerous failure modes in results interoperability.
Validation Workflow for Safe ORU Mapping
Validation should include structure, terminology, and clinical meaning. Start with raw message inspection in the HL7 Viewer so you know exactly which OBR and OBX fields are populated. Then map the same message in the HL7 v2 to FHIR Mapper and confirm that every clinically important element survives: subject, encounter, report code, observation codes, value types, units, abnormal flags, and status.
Use message sets that include final, corrected, textual, numeric, coded, and panel-style results. Confirm that a corrected ORU updates the existing report lineage rather than duplicating it. Compare your implementation behavior against the broader migration guide, and keep the companion ADT mapping article close by because result linkage to Patient and Encounter is only as strong as the event model underneath it.
Implementation Checklist Before Production
- Define how OBR groups become DiagnosticReport resources.
- Map OBX-2 value types explicitly rather than coercing all values to text.
- Preserve local and standard code systems honestly.
- Implement correlation keys for corrected and repeat result handling.
- Validate units, abnormal flags, and reference ranges because they drive downstream meaning.
- Test panel, narrative, and microbiology style messages, not only simple chemistry results.
Conclusion
ORU to FHIR mapping succeeds when teams preserve both the report-level story and the individual result-level detail. DiagnosticReport gives structure to the result event, while Observation holds the discrete clinical facts that applications search, graph, and interpret. The transformation only becomes trustworthy when value types, status history, units, reference ranges, and identifier-based correlation are handled deliberately rather than incidentally.
Use the HL7 Viewer to understand the source message, validate bundle output in the HL7 v2 to FHIR Mapper, and read this together with the companion guide on ADT to Patient and Encounter mapping so your event and result layers stay aligned. The examples here are educational and should be validated against local implementation guides, terminology policies, and clinical governance requirements before production deployment.